Posted by American Heart Association on Oct 25th 2020
2020 AHA Advanced Cardiac Life Support (ACLS) Guidelines
2020 AHA Advanced Cardiac Life Support (ACLS) Guidelines
Adult Cardiac Arrest Algorithm
The Adult Cardiac Arrest Algorithm was modified to emphasize the role of early epinephrine administration for patients with nonshockable rhythms.
Changes include:
- Amiodarone and lidocaine are now equivalent as antiarrhythmics in cardiac arrest
- Added a step to consider appropriateness of continued resuscitation
- Moved epinephrine to as soon as possible for nonshockable rhythms to emphasize early administration after starting CPR

Post–Cardiac Arrest Care Algorithm
The Post–Cardiac Arrest Care Algorithm is updated to emphasize the need to prevent hyperoxia, hypoxemia, and hypotension.
Changes include:
- Oxygen saturation of 92% to 98%
- Separated out initial stabilization phase to include “Manage airway,” “Manage respiratory parameters,” and “Manage hemodynamic parameters”
- Added step to consider emergent cardiac interventions
- Added “Obtain brain CT,” “EEG monitoring,” and “Other critical care management” if patient is comatose
- Added guidance on reversible etiologies
- Removed Doses and Details boxes on right
- Added sections on Initial Stabilization Phase and Continued Management and Additional Emergent Activities on right

Adult Bradycardia Algorithm
Changes include:
- Atropine dose changed from 0.5 mg to 1 mg
- Dopamine dose changed from 2-20 mcg/kg per minute to 5-20 mcg/kg per minute
- Under “Identify and treat underlying cause,” added “Consider possible hypoxic and toxicologic causes”
- Under “Atropine,” transcutaneous pacing has “and/or” for dopamine or epinephrine (changed from “or”)

Acute Coronary Syndromes Algorithm
An updated algorithm is provided for acute coronary syndromes.
Changes include:
- Upon EMS arrival at the hospital, transport to the emergency department or cath lab per protocol. Best practice is to deliver directly to the cath lab, as long as personnel are present for the procedure, to shorten the time to treatment
- First medical contact–to–balloon inflation (percutaneous coronary intervention) goal of 90 minutes or less
- 12-lead electrocardiographic analysis is now classified into 2 main categories, ST-segment elevation myocardial infarction (STEMI) and non–ST-segment elevation acute coronary syndromes (NSTE-ACS). NSTE-ACS has 2 branches under it, attempting to have emergency departments conduct further testing before release

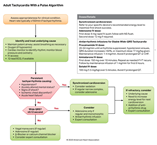
Adult Tachycardia With a Pulse Algorithm
The Adult Tachycardia With a Pulse Algorithm includes updates to IV access and synchronized cardioversion.
Changes include:
- Moved IV access and 12-lead ECG to step 2 (earlier in the algorithm)
- Added step 5 to guide on what to do if refractory (if synchronized cardioversion is not working, or if have wide QRS and adenosine/antiarrhythmic infusion is not working)
Cardiac Arrest in Pregnancy In-Hospital ACLS Algorithm
A revised algorithm is provided for cardiac arrest in pregnancy.
Changes include:
- Layout is more streamlined
- Added step for administering 100% O2 and avoiding excessive ventilation
- Removed step to assess for hypovolemia/treatment
- Changed “If no ROSC in 4 minutes” to “5 minutes”
- Maternal Cardiac Arrest box that highlights:
- Team planning
- Priorities of high-quality CPR and relief of aortocaval compressions with lateral uterine displacement
- Goal of perimortem cesarean delivery
- Deliver in 5 minutes (depending on provider resources and skill sets)

Adult Suspected Stroke Algorithm
An updated algorithm is provided for adult suspected stroke.
Changes include:
- EMS should now use a stroke severity tool after performing a stroke screening to determine if a large-vessel occlusion exists
- New EMS stroke routing algorithm should be used to determine the hospital destination
- Upon EMS arrival at the hospital, transport to the emergency department or imaging lab per protocol. Best practice is to deliver directly to the imaging lab to shorten the time to treatment
- Patients can be treated with alteplase and endovascular therapy if time goals are met and contraindications do not exist
- The window for conducting endovascular therapy has been extended to up to 24 hours

Neuroprognostication
A visual aid is provided to guide and inform neuroprognostication.
Because any single method of neuroprognostication has an intrinsic error rate and may be subject to confounding, multiple modalities should be used to improve decision-making accuracy.

Physiologic Monitoring of CPR Quality
2020 (Updated): It may be reasonable to use physiologic parameters such as arterial blood pressure or end-tidal CO2 when feasible to monitor and optimize CPR quality.
2015 (Old): Although no clinical study has examined whether titrating resuscitative efforts to physiologic parameters during CPR improves outcome, it may be reasonable to use physiologic parameters (quantitative waveform capnography, arterial relaxation diastolic pressure, arterial pressure monitoring, and central venous oxygen saturation) when feasible to monitor and optimize CPR quality, guide vasopressor therapy, and detect ROSC.
Why: Similar to the above, although the use of physiologic monitoring such as arterial blood pressure and/or end-tidal CO2 to monitor CPR quality is an established concept, new data support its inclusion in the Guidelines. Data from the AHA Get With the Guidelines-Resuscitation registry show higher likelihood of ROSC when CPR quality is monitored by using either end-tidal CO2 or diastolic blood pressure. This monitoring depends on the presence of an endotracheal tube or arterial line, respectively. Targeting compressions to an end-tidal CO2 value of at least 10 mmHg, and ideally 20 mm Hg or greater, may be useful as a marker of CPR quality. An ideal target has not been identified.
Double Sequential Defibrillation Not Supported
2020 (New): The usefulness of double sequential defibrillation for refractory shockable rhythm has not been established.
Why: Double sequential defibrillation is the practice of applying near-simultaneous shocks with 2 defibrillators. Although some case reports have shown good outcomes, a 2020 ILCOR systematic review found no evidence to support double sequential defibrillation and recommended against its routine use. Existing studies are subject to multiple forms of bias, and observational studies do not show improvements in outcome. A recent pilot randomized clinical trial suggested that changing the direction of defibrillation current by repositioning the pads may be as effective as double sequential defibrillation, while avoiding the risks of harm from increased energy and damage to defibrillators. Based on current evidence, it is not known whether double sequential defibrillation is beneficial.
Intravenous Access Preferred Over Intraosseous
2020 (New): It is reasonable for providers to first attempt establishing IV access for drug administration in cardiac arrest.
2020 (Updated): IO access may be considered if attempts at IV access are unsuccessful or not feasible.
2010 (Old): It is reasonable for providers to establish IO access if IV access is not readily available.
Why: A 2020 ILCOR systematic review comparing IV vs IO (principally pretibial placement) drug administration during cardiac arrest found the IV route was associated with better clinical outcomes in 5 retrospective studies; subgroup analyses of RCTs that focused on other clinical questions found comparable outcomes when IV or IO was used for drug administration. Although IV access is preferred, there are situations in which IV access is difficult, and in such situations IO access is a reasonable option.
Do Not Use Point-of-Care Ultrasonography for Prognostication During Resuscitation
2020 (New): The AHA suggests against the use of point-of-care ultrasound for prognostication during cardiopulmonary resuscitation. This recommendation does not preclude the use of ultrasound to identify potentially reversible causes of cardiac arrest or detect ROSC.
2020 (New): If an experienced sonographer is present and use of ultrasound does not interfere with the standard cardiac arrest treatment protocol, then ultrasound may be considered as an adjunct to standard patient evaluation, although its usefulness has not been well established.
Why: Point-of-care cardiac ultrasound can identify cardiac tamponade or other potentially reversible causes of cardiac arrest and identify cardiac motion in patients with pulseless electrical activity. However, cardiac ultrasound is also associated with longer interruptions in chest compressions. A single small RCT found no improvement in outcomes with use of cardiac ultrasound during CPR. A recent systematic review found that no sonographic finding had consistently high sensitivity for clinical outcomes to be used as the sole criterion to terminate cardiac arrest resuscitation.
Care and Support During Recovery
2020 (New): The AHA recommends that cardiac arrest survivors have multimodal rehabilitation assessment and treatment for physical, neurologic, cardiopulmonary, and cognitive impairments before discharge from the hospital.
2020 (New): The AHA recommends that cardiac arrest survivors and their caregivers receive comprehensive, multidisciplinary discharge planning, to include medical and rehabilitative treatment recommendations and return to activity/work expectations.
Why: The process of recovery from cardiac arrest extends long after the initial hospitalization. Support is needed during recovery to ensure optimal physical, cognitive, and emotional well-being and return to social/role functioning. This process should be initiated during the initial hospitalization and continue as long as needed. These themes are explored in greater detail in a 2020 AHA Scientific Statement (Sawyer 2020).
Ventilation in Respiratory and Cardiac Arrest
Respiratory Arrest: If an adult victim with spontaneous circulation (ie, strong and easily palpable pulses) requires support of ventilation, it may be reasonable for the healthcare provider to give rescue breaths at a rate of about 1 breath every 6 seconds, or about 10 breaths per minute.
Cardiac Arrest: It may be reasonable for EMS providers to use a rate of 10 breaths per minute (1 breath every 6 seconds) to provide asynchronous ventilation during continuous chest compressions before placement of an advanced airway. If an advanced airway is in place, it may be reasonable for the provider to deliver 1 breath every 6 seconds (10 breaths/min) while continuous chest compressions are being performed.
Why: Studies have indicated that one breath every 6 seconds (10 breaths per minute) improve survival and neurological outcomes.
Epinephrine Administration
For educational purposes, healthcare providers can administer epinephrine by using a mid range of every 4 minutes to match every other rhythm check.
Oxygen Administration
Greater than 94% for stroke and general care.
92% to 98% for post–cardiac arrest care.